Introduction

https://www.ft.com/content/6f43b13c-fbdb-11e5-8f41-df5bda8beb40
Copper is an essential metal necessary for bodily functions. It has been used for centuries and is present in water and food. It is also necessary for the function of many enzymes in the body (Casarett & Doull). It is also naturally present in sediment, soil, plants, and air and is currently used in the production of many metal products. In addition, it is found in metal mixtures, such as bronze and brass (CDC Copper Toxicological Profile).
Biotransformation
Copper has the ability to rapidly enter the bloodstream upon absoprtion. It is transferred to many organic ligands in the body such as imidazole groups on amino acids. In many tissues, copper binds to metallothionen and other copper dependent enzymes. Excretion occurs mainly via bile, but can also occur with urine and feces (CDC Copper Toxicological Profile).
Below is an illustration describing the metabolism of copper:

http://www.eurowilson.org/en/living/guide/pathway/index.phtml
Toxicokinetics
Over half of an oral dose of copper (55-75%) is absorbed from the GI tract. Copper is mainly stored in the liver and brain. The amount of copper in the body stays relatively constant through several mechanisms including copper ATPases interacting with chaperone proteins, intestinal reabosorption, and enterhepatic recirculation. The limit for daily consumption is 10mg. Ingesting copper salts in large quantities can lead to death of liver cells.
Source: Casarett & Doull

https://accesspharmacy.mhmedical.com/content.aspx?bookid=958§ionid=53483748
Mechanism of Action/Target Organs
Copper is able to rapidly oxidize and reduce between Cu(I) and Cu(II) and is involved in redox reactions, however this can also cause production of free radicals which can lead to toxic effects. Copper is initially bound to intestinal cells due to going through the GI tract. After being released, it is transported to the liver while bound to albumin and is then distributed to tissues and organs (CDC Copper Toxicological Profile).
The main target organs include the liver and brain (Cassarett & Doull).

https://www.organic-chemistry.org/namedreactions/ullmann-reaction.shtm
Carcinogenecity
Many studies have been preformed to determine the carcinogenicity of copper after oral exposure and parenteral administration in humans and animals. Studies in male Winstar rats following parenteral administration did not yield significant results but an increase of hepatocellular carcinomas was found in Long-Evans Cinnamon rats. No carcinogenic effects have been found in humans (CDC Copper Toxicological Profile).
Genetic Susceptibility/Heritable Traits
There are some heritable diseases that deal with copper metabolism
Menkes Disease: sex-linked genetic disorder in which male infants have copper deficiency, leading to several symptoms such as mental retardation, connective tissue dysfunction, and white matter degeneration. The gene associated with this is the ATP7A gene and is involved with the copper transport. Issues in transport lead to too much copper in enetrocytes.

https://ghr.nlm.nih.gov/condition/menkes-syndrome
Wilson Disease: autosomal recessive disorder dealing with too much copper in kidneys, liver, and the brain. This is due to impaired copper metabolism and transport and is due to mutations on chromosome 13 on the Wilson disease locus, which encodes ATP7B, an ATPase.

http://www.eurowilson.org/en/living/guide/what/index.phtml
Hereditary Aceruplasminemia: autosomal recessive disorder which leads to increased iron levels. It is due to a mutation in the gene encoding for ceruplasmin, a copper binding protein.
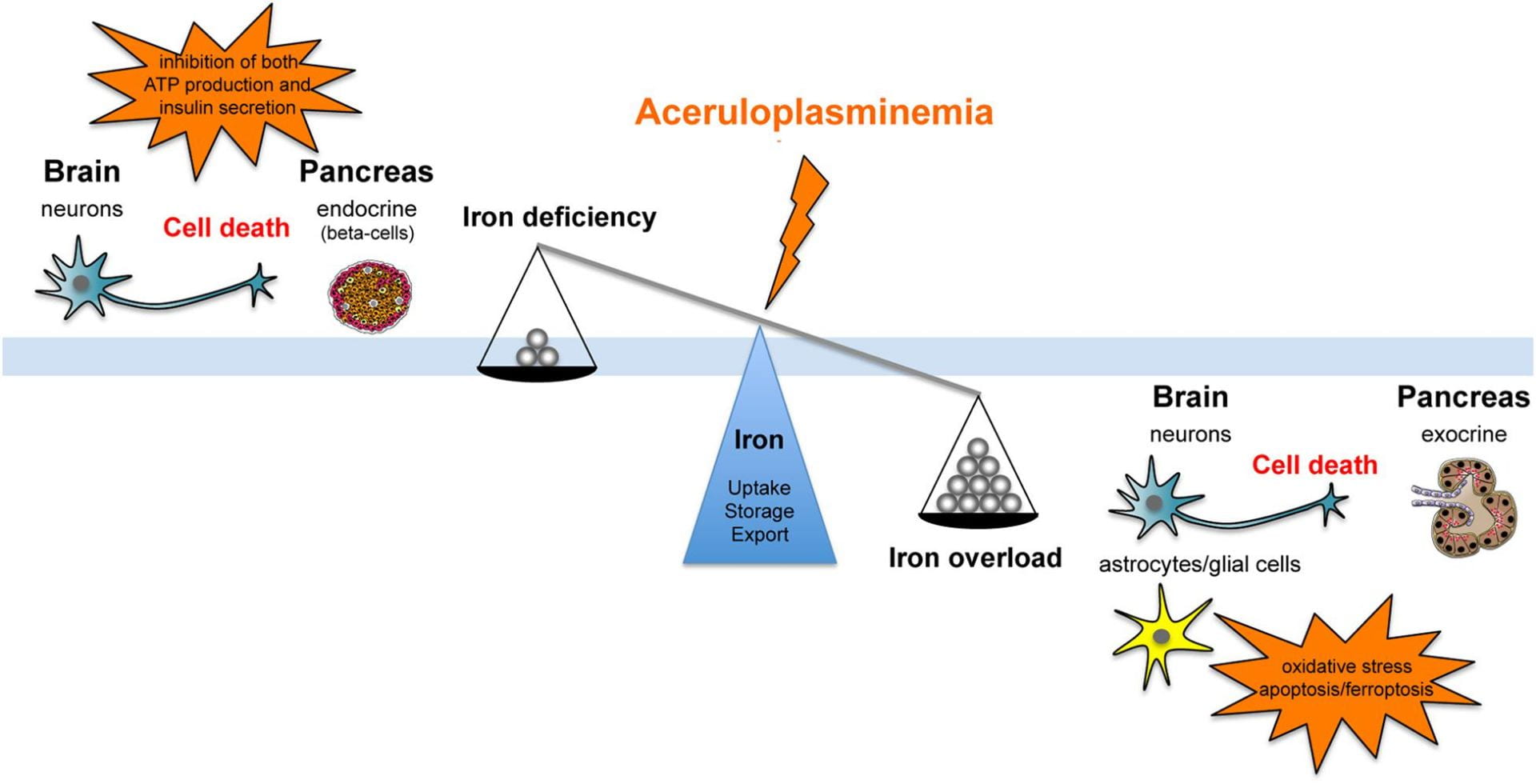
https://www.frontiersin.org/articles/10.3389/fnins.2018.00903/full
Source: (Cassarett & Doull)
Treatment
Treatment of disorders can include administration of zinc salts and chelators. An example of this is d-penicillamine.

https://www.nature.com/articles/s41598-018-22511-6

https://www.buy-pharma.md/Penicillamine-p-1481.html
Source: Cassaret & Doull
Signs and Symptoms of Toxicity
Liver damage
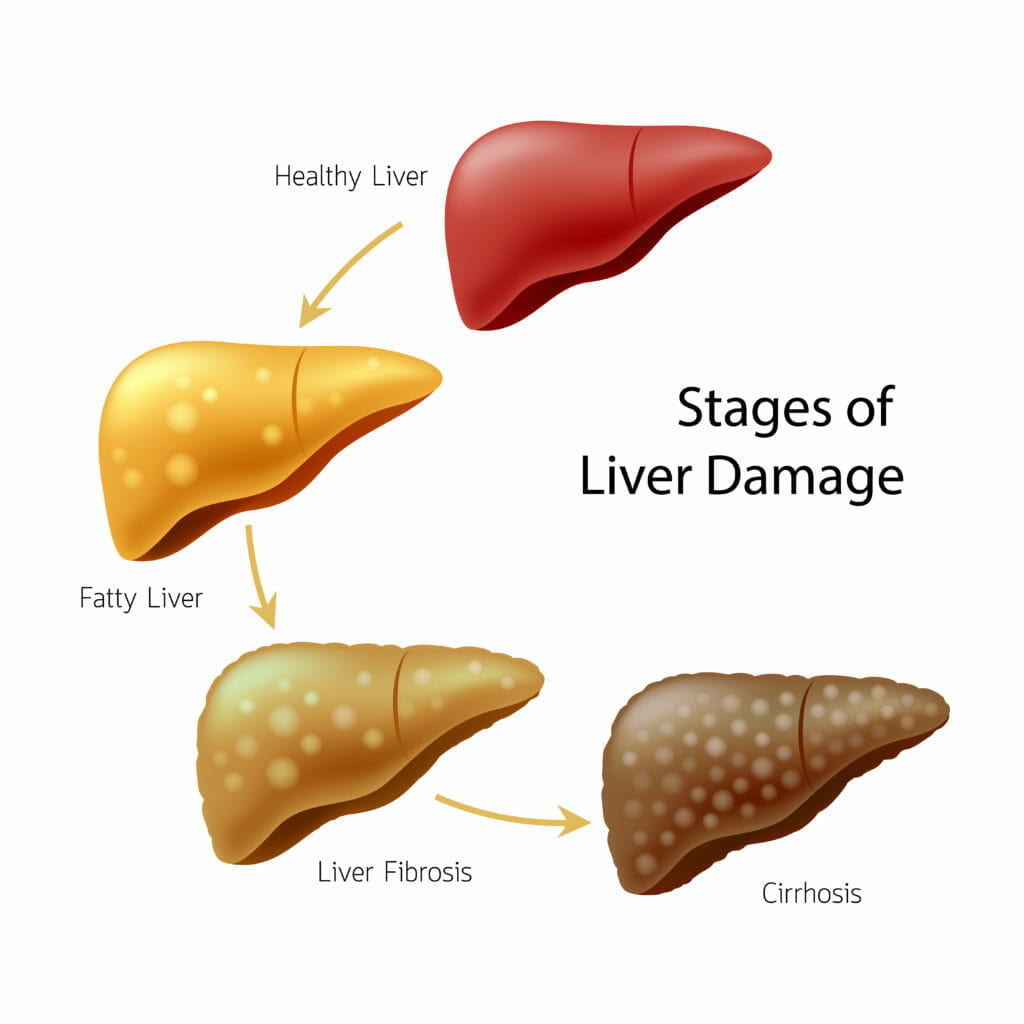
https://family-intervention.com/blog/recognizing-early-symptoms-of-liver-disease/
GI Symptoms (ie-abdominal pain, vomiting, nausea, cramps)

https://www.belmarrahealth.com/type-1-diabetes-gastrointestinal-symptoms-cause-identified-treatment-possible/
Source: Copper Fact Sheet
Biomarkers
Copper induced liver damage causes changes in serum enzymes, such as alanine aminotransferase, aspartate, and alkaline phosphate. Another biomarker is increases in bilirubin levels. A decrease in metalloenzymes and cytochrome oxidase are associated with reduced levels of copper.
https://www.phrma.org/fact-sheet/biomarkers-and-surrogate-endpoints
Source: CDC Copper Toxicology Profile
Essentiality/Deficiency
Copper is necessary for the functioning of many metalloenzymes including oxidases. These enzymes are important for energy metabolism and redox reactions. Low levels of copper result in several symptoms including bone abnormalities and hypochronic, microcytic anemia.

https://naturallyhealthynews.com/articles/healtharticles/9-signs-you-are-experiencing-copper-deficiency/
Source: Cassaret & Doull