Teamwork is critical in the practice of medicine, nowhere more than in the ICU. I did my sub-internship in the neurocritical care unit (NCCU) at OSU. I had several patient experiences that touched me but the memories that I carry with me are mostly from my teammates. In the ICU more than other places in the hospital, nurses, respiratory therapists, residents, advanced practice nurses, and attendings work closely together to save lives. I was struck by the efficiency of communication in the unit. A standard method to round, to run a code, and to handoff is key to the success of the systems-based practice in the ICU.
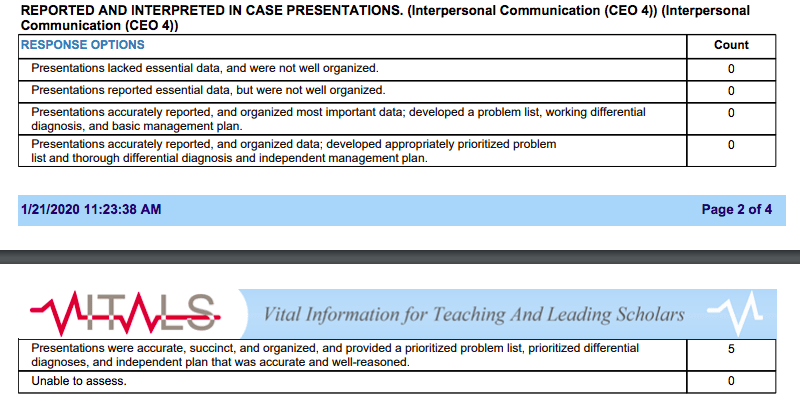
Rounding in the NCCU is handled differently than in other parts of the hospital. The nursing staff leads, reading off data and giving report of overnight events system-by-system of the body. The residents, medical students, and fellows can interject with information as needed, but the attending hears the information from the primary source, the nurse who has been taking care of the patient. The nursing staff interacts the most with the patients, they manage the drips and the lines, they are the first line. This method of rounding leads to very effective patient care. There is no debate about what the patient has been getting or what their status is because the information comes direct. The system is designed for maximum efficiency in communication and it leads to excellent medical practice.
I saw two codes run while I was in the unit and both were run very well. An APP ran both codes that I witnessed, in total command of the team she was running. Codes are run with a standard practice to give the patient the best chance. The pharmacist handles the drugs, the nursing staff handles compressions and note taking, the PCAs run and get supplies, and every member of the team supports one another. I appreciated the rhythm that the codes had, despite the differences in the patients, they were both run the same way. When I am an intern, and I have to run the code, I will take comfort in that every code should have similar features and that each member of the team should support one another.
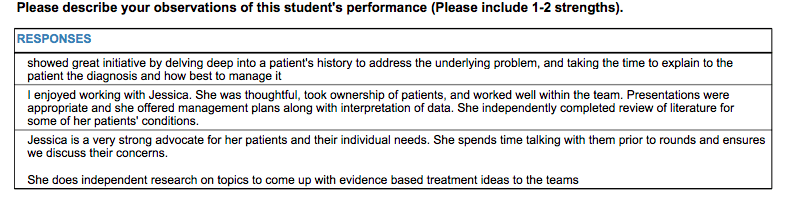
The final system in place in the ICU that I observed as being critically important was the handoff system. Due to duty hour restrictions every member of the team needs to handoff to night shift. In the ICU where every patient is sick, it is doubly important for the day team to have a plan in place and to communicate it effectively to their colleagues. This is an activity that sub-I’s are encouraged and required to participate in. At first, I had no idea which information was important and which was not. But throughout the rotation with instruction from my residents and from experience, I learned what was important for the night team to know. My evaluations reflected that growth as it was noted that I communicated effectively. I will continue to work on this skill and others, such as documentation, when I become an intern next year.