Differential Diagnosis for UTI
Differential Diagnosis I and Final Diagnosis:
UTI
Rationale:
Mrs. Smith’s presentation of symptoms such as abdominal pain, back pain, urinary frequency with little urine being made, dysuria, and foul-smelling urine provide rationale that this could be a Urinary Tract Infection. A UTI is an infection of the urinary tract infection that can happen when bacteria from the rectum populates in any part of the urinary tract system, including the urethra and ureters and can also move up to the bladder and kidneys. She participates in spinning class which could contribute to getting a UTI. Mrs. Smith has had a recent URI and was receiving antibiotics and she is also a Type I diabetic. She is also sexually active. All of these provide rationale to support this could be a potential UTI.
- Women are at higher risk for urinary tract infections due to their anatomy. The urethra is shorter and bacteria can more easily travel to the bladder. The anus is also located closer to the urethra than in men, therefore the bacteria is able to more easily move to the urethra from the anus.
- Migration of bacteria can happen from improper wiping after bowel movement and sexual activity.
- Spin class activity can contribute to UTI if Mrs. Smith is not changing out of her clothes after her workout. Sweat and moisture can cause bacteria to grow, causing a UTI.
The rationales listed above support the diagnosis of UTI, but there are several different diagnoses listed below that are reasonable possibilities. (McCance & Huether, 2019).
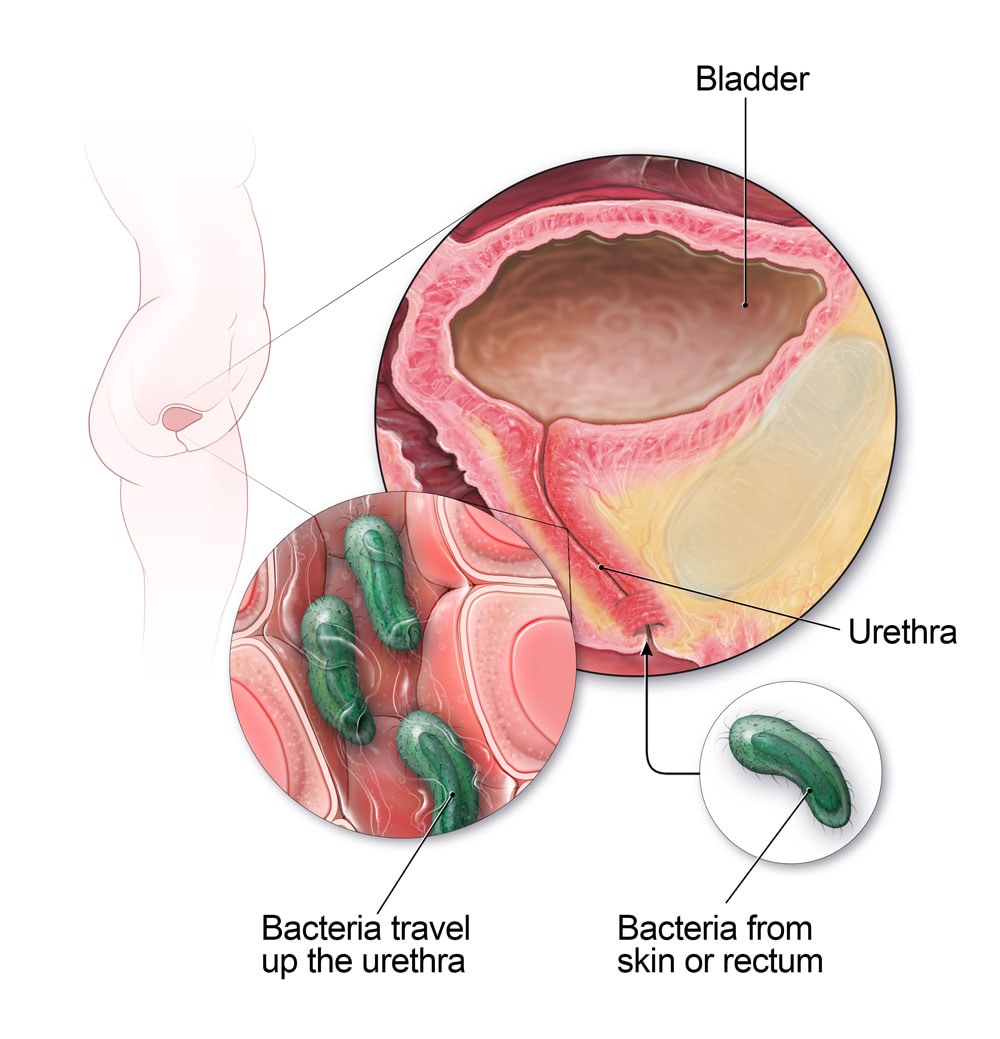 Image retrieved from https://www.cdc.gov/antibiotic-use/community/for-patients/common-illnesses/uti.html
Image retrieved from https://www.cdc.gov/antibiotic-use/community/for-patients/common-illnesses/uti.html
Differential Diagnosis II:
Pregnancy
Rationale:
Mrs. Smith’s history states that she is a sexually active, married, 27 year old who has a 3 year old child. This history is important because it leads us to believe that ruling out pregnancy would be reasonable in this scenario.
- Pregnancy contributes to an increase in susceptibility of UTIs
- There is an increase in bladder volume and a coexisting decrease in detrusor tone
- progesterone can cause ureteric dilation due to relaxation of smooth muscle and the gravid uterus can also compress the ureters causing hydronephrosis
- In pregnancy, the kidney allows in more glucose, causing an increase in bacteria growth
- Pregnancy alters the immune response and can increase the risk of infection (Curtiss & Duckett, 2017).
Mrs. Smith could be experiencing an early sign of pregnancy presenting with UTI symptoms, and this should be ruled out as she is within child bearing age and has had a previous pregnancy. She also states she is sexually active with the use of spermicide, so history on proper use of spermicide should be evaluated.
Differential Diagnosis III:
Nephrolithiasis (Kidney Stones)
Rationale:
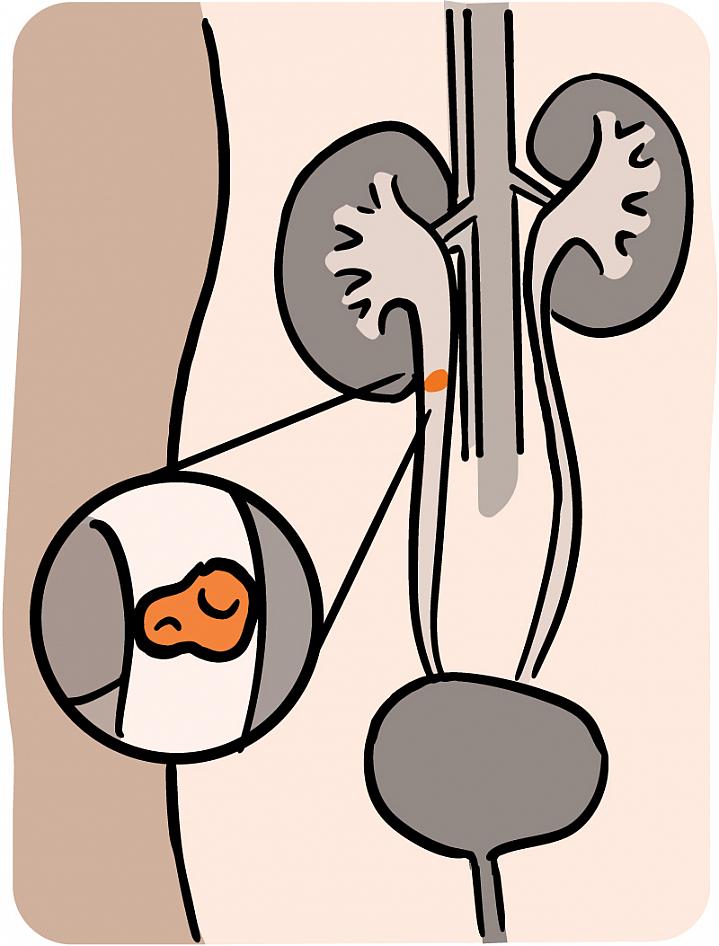
Mrs. Smith presents with abdominal pain 4/10 and complains of lower back pain. She is also complaining of frequency to void with little urine made. Kidney stones can present with similar symptoms to the ones that Mrs. Smith is describing. Kidney stones occur when masses of crystals, proteins, or other substances are formed and stored in the kidneys (McCance & Huether, 2019).
- Pain that radiates to the lateral flank or lower abdomen typically indicates obstruction in the midureter, and includes bothersome lower urinary tract symptoms.
- Lower urinary tract symptoms include urgency, frequency, and urge incontinence
- Microscopic hematuria may be present
With the symptoms listed above relating to kidney stones, and the symptoms that Mrs. Smith is presenting with, there is reasonable rationale to rule out kidney stones as a possible differential diagnosis. More detailed history can be taken to help rule out stones such as diet and any history of previous kidney stones. (McCance & Huether, 2019). In Mrs. Smith’s case, this an unlikely cause of her symptoms, as she is denying nausea, vomiting, and a fever. Kidney stones typically present with these as well.
 (NIH, 2017).
(NIH, 2017).
Image retrieved from https://ghr.nlm.nih.gov/condition/kidney-stones#resources
Differential Diagnosis IV
STI
Rationale:
Mrs. Smith presents with painful urination, frequency, and foul-smelling urine. She reports abdominal pain on a scale 4/10. She also states that she is sexually active with her husband and they use spermicide as birth control. She has a past medical history of chlamydia when she was 19. STIs such as gonorrhea and chlamydia occur after a sexual act with an infected partner. The bacteria is passed from the affected partner to the other. The transmission occurs when there is contact of epithelial surfaces such as occurs during vaginal, oral, or anal intercourse, and infection in adults can be maintained in the vagina, rectum, oropharynx, or urethra (McCance & Huether, 2019).
- Gonorrhea in women can present with dysuria, abnormal menses, dyspareunia, lower abdominal/pelvic pain, and fever.
- Chlamydia infections present symptoms that are closely parallel to those of gonorrhea.
- Gonorrhea and chlamydia are both present in the urinary tract, as well as the higher reproductive organs, if left untreated.
- Both are sexually transmitted infections that occur in men and women and present with a multitude of symptoms, including the ones listed above.
Sexually transmitted infections can cause symptoms stated above that can present similarly to UTIs. With sexual activity, previous history, and present symptoms, underlying STI could potentially be the cause of her presenting symptoms (McCance & Huether, 2019).

Image retrieved from https://americanpregnancy.org/womens-health/gonorrhea/