Guys. You, ahem, made it rain on my birthday. Knowing I’m surrounded by people who believe in me and what I do is the BEST gift I could ask for and I can’t thank you all enough.
Immediate costs of the project are covered, but the longer we can pay our own way in staff salaries and supplies, the better for CLI. They will pick up the expenses when my contributions run out, but that does take away from other funds they would otherwise use to care for the community and execute other important research projects in the catchment area.
So in case you haven’t made it over to my fundraising page yet, I’m keeping it open through this month.

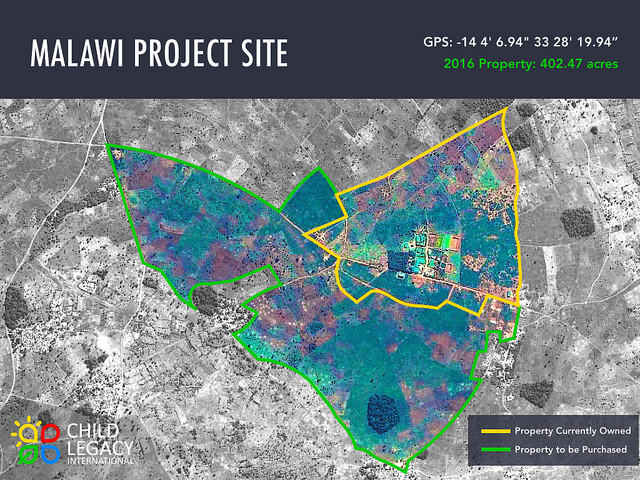
My advisor took a good hard look at our materials and started asking the what-ifs and other awesome questions that will make my tools more powerful. Grateful for the close look but I have a lot of the more tedious work that’s not so fun to blog about. Instead of boring you to death about my spreadsheets and protocols, I want to tell you more about the site I’m working at, Child Legacy International.
Just from looking at photos you get the impression that there’s a lot going on in this compound in rural Malawi.

First, it runs off of wind and solar power. When you run a clinic and research lab, having consistent power supply is not an option, so they’re building a pretty robust system. When I met one of the founders a couple of months ago, he made a good point about providing creature comforts as incentives to retain the Malawian staff they train and educate to work at the center. I get it, too–those little things count and you want to have the best people.
Though my project is really focused on work for the McGuire Wellness Center, CLI is way more than just a clinic.

Their compound has farms,

including tilapia ponds that feed staff and patients, then extra go to market for profit to the center

clean water access projects,

below is a photo of the cofounder I haven’t met yet–from what i can see in the photos she walks the walk when it comes to collaborative efforts and i love it.

There’s also a school for young kids, and opportunities for vocational training too.

plus a lab for bio testing, a pharmacy, a research arm, so much!

It’s impressive to peruse their photos and see how much they have going on, and to see their plans in the future.
The more I learn about this organization the happier I am to get this opportunity to work with them. I was also glad to see that they’ve earned the highest possible rating by Charity Navigator. It’s another reason why I want to support my surveillance system for as long as possible. The money that’s being put to work by this organization is used where it’s needed and it’s used efficiently.
Thanks for all of the support you’ve all shown me already, and for any new supporters reading this now!






