In this article I explain the neurological mechanisms that lead to depression, from an anato-structural standpoint. Depression is a major hindrance for concentration and appropriate study. Understanding how it takes place is essential for the depressed individual, to overcome it and become a better learner.

Alenushka, by Victor Vasnetsov (1881).
The Effect of Amygdala Abnormalities on
Generalized Anxiety Disorder and Major Depression
Angelo Juarez
The amygdala, an element of the limbic system, is a structure located on the inner and medial portion of both temporal lobes of the brain. It is present not only in humans, but also on nonhuman primates, among other higher vertebrates. In humans it has a volume of about 2.0 cm3, making up only 0.3% of the average brain size volume (~1,300 cm3), and contains the nuclei of roughly 12 million neurons on each side, which is also a small amount in comparison to around 100 billion neurons in the entire brain. Nonetheless, it is presumed the amygdala plays an important role in nearly every neuropsychiatric disorder, in part because of the high level of neural connectivity it has to other structures in the brain (Figure 1). The complex neural interconnections attained by the amygdala give birth to the conjunction of neurological processes known as emotions, most notably fear, aggression and anxiety, and in doing so, it regulates cognitive function. This structure also has a crucial role in memory processing and decision-making. The first research done to understand the role of the amygdala began in the late 19th century, when, in 1888, Brown and Schaefer first performed experiments in rhesus monkeys. Later, a series of studies in nonhuman primates, which involved brain lesion techniques as well as non-invasive procedures, led to the understanding that the amygdala plays an essential role in the identification of dangerous situations, social behavior, temperament, vigilance and fear. Likewise, these studies concluded that the amygdala has a crucial involvement in both generalized anxiety and major depression, two closely related mental disorders which constitute the most common psychiatric ailments among young and adult people, with a lifetime incidence of 33.7% for any kind of anxiety disorder and 18.3% for major depressive disorder. Their relationship is also striking, as anxiety disorders have an onset during preadolescent years and are usually followed by the emergence of major depression during adolescence or early adulthood (Amaral & Adolphs, 2016). Based on these findings, it is plausible to asseverate that amygdala structure and function can deeply affect cognitive and behavioral response, leading to generalized anxiety disorder and major depression. Addressing these two disorders is of great importance and understanding their underlying neuroanatomical processes could bring about improvements in pharmaceutical development and therapeutic techniques.

Figure 1. Schumann, C.M., Vargas, M.V., Lee, A. (2016) Extrinsic amygdala connectivity, [Figure]. From Living Without an Amygdala (pg. 56), by Amaral, D.G., Adolphs, R., 2016, New York: The Guildford Press.
Both fear and anxiety must be understood to comprehend the different types of anxiety disorders. Fear is a state of immediate alarm due to a clearly-defined source of danger, and it is focused on the present. On the other hand, anxiety is a sense of uneasiness amidst a vague or unclear source of danger, or to the feeling of uncertainty, and it is focused on the future. Fear and anxiety are responsible for cautious behavior, preventing outcomes that could affect the integrity of an individual, therefore, they serve an organism by protecting it from dangerous situations. It is when these emotions are excessive, uncontrolled, or enkindled inappropriately, that they become abnormal, impairing an organism from developing regular daily activities (Comer, 2015; Forster, Novick, Scholl & Watt, 2012). The current classification of anxiety disorders comprises seven pathologies, which include the following: generalized anxiety disorder (GAD), obsessive-compulsive disorder (OCD), posttraumatic stress disorder (PTSD), specific phobias, social anxiety disorder (SAD), panic disorder and agoraphobia. From these, the first two are characterized by anxiety, while the remaining five are typified by an element of fear (Forster, Novick, Scholl & Watt, 2012).
Studies in nonhuman primates have shown that the amygdala plays a crucial role in normal fear and the processing of emotions, while there has been reports of anxious behavior in individuals with altered amygdala function. As mentioned previously, a history of anxiety that dates back to preadolescent years is common and it is believed that this early onset of anxiety is due to morphophysiological alterations in the central extended amygdala, which is a hypothetical anatomical complex that needs further investigation, but which is thought to constitute an element of the basal forebrain, a macro structure that comprises highly interconnected elements, such as the cholinergic nucleus basalis of Meynert and the ventral striatopallidal system. Yet there is still a need for further research to better comprehend morphophysiological amygdala alterations that lead to childhood anxiety. Another important finding from studies done in rhesus monkeys is that anxious phenotype is heritable and closely linked to variations in the central nucleus of the amygdala (Ce) (Figure 2). Also, these studies have demonstrated that amygdala activation can be decreased with the intake of anxiolytics in a dose-dependent manner (Amaral & Adolphs, 2016).
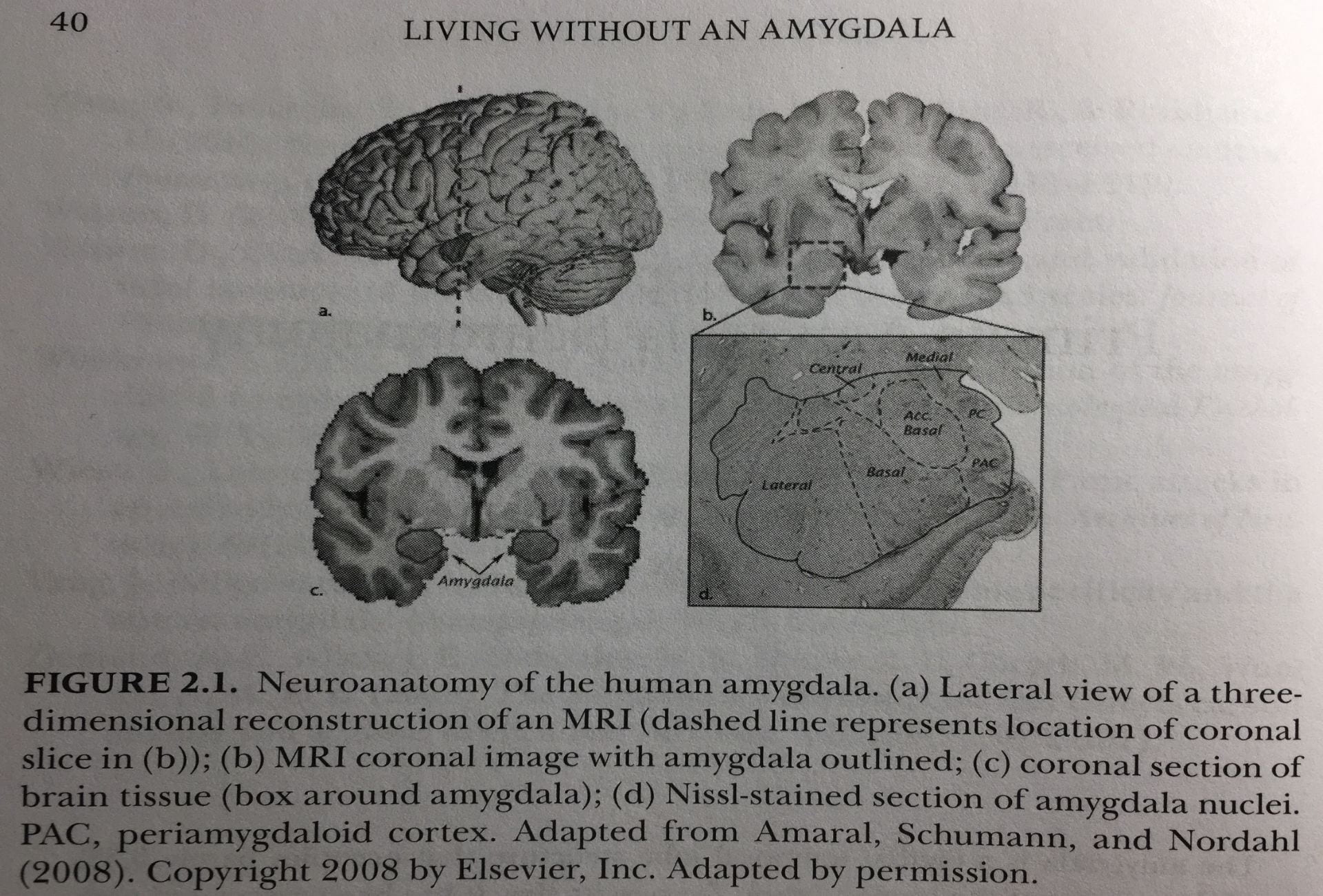
Figure 2. (a) Lateral view of a three-dimensional reconstruction of a human brain MRI, where the dashed line represents a coronal cut seen in (b)); (b, c) MRI coronal image showing and outline of amygdalae in the human brain. (d) Nissl-stained section of human amygdala nuclei. PC, piriform cortex. PAC, periamygdaloid cortex. Schumann, C.M., Vargas, M.V., Lee, A. (2016) Neuroanatomy of the human amygdala, [Figure]. From Living Without an Amygdala (pg. 40), by Amaral, D.G., Adolphs, R., 2016, New York: The Guildford Press.
Kalin and Shelton developed, in the year 1989, a three-stage behavioral essay for young rhesus monkeys with anxious temperament (AT), designated as the ‘human intruder paradigm,’ to better understand behavioral inhibition (BI) in human children (an early predictor of SAD), through key parallelisms in behavior with these animals. The experiment initially consisted in selecting a subject from a cage where it was initially accompanied by other cage mates and then placed in another one where it remained alone, also in an empty room. Initially, while being alone, the monkey would start exploring the cage while emitting ‘coo’ calls, which was interpreted as a way to call their mothers or other conspecifics for help. In a second scenario, when exposed to a human intruder that would not engage in direct eye contact but, instead, would show his profile (no eye contact, NEC), the monkey would focus its attention to him, by hiding and remaining still as if avoiding being seen, a reaction termed freezing. In the third stage of the experiment, the intruder would enter the room and stare the monkey directly in the eye, often educing aggressive behavior in the experimental subject, such as gibbering and cage rattling. Later, more researchers contributed to the human intruder paradigm behavioral essay, by proving that diazepam decreased NEC-induced freezing in rhesus monkeys, while beta carboline, an anxiogenic benzodiazepine inverse agonist, had the opposite effect. Other scientists observed increased levels of serum cortisol/increased pituitary-adrenal response after induced threat in the subjects. Most importantly, further research, involving post NEC-induced freezing/brain PET scan measurements of blood-infused radiotracer 18-fluorodeoxyglucose, demonstrated increased amygdala activity to novelty and potential threat, as well altered functional connectivity between the amygdala and prefrontal cortex, in rhesus monkeys with anxious temperament. There is extensive evidence that these amygdala abnormalities are heritable in both human and non-human primate models (Amaral & Adolphs, 2016).
Induced amygdalar lesion studies in rhesus monkeys, as well as human clinical cases of amygdalar damage due to neurological disease, have likewise associated the amygdala to anxious temperament. The generated damage decreased fearfulness and demureness in response to dangerous situations in the animal model and modified stress-induced cortisol release by the pituitary-adrenal axis. When amygdalar damage is seen in humans, it presents itself as a decrease in anxiety in social situations where anxious temperament would be expected to occur. In a famous clinical case, a female patient who suffered from Urbach-Wiethe disease, a rare recessive genetic disorder that produces generalized thickening of the skin and mucous membranes, and in her case, amygdala calcification, developed symptoms of fear and anxiety disinhibition, including an increased ability to trust and approach strangers, an inability to recognize signs of fear in others, a lack of recognition for interpersonal space, and an incapability for Pavlovian fear conditioning (Amaral & Adolphs, 2016).
It is known that much of the amygdala develops during the first seven years of life in humans. By the fourth year of life, this structure is almost completed. Because of this early development of the amygdala it is believed that the early years of neurological development are crucial for its appropriate functioning during adulthood. Research performed in the animal model has shown that induced trauma during early mouse and non-human primate development can bring about noticeable deficits in amygdala function, leading to anxious behavior in early youth and ensuing depression starting in adolescence, and has suggested that the basolateral nucleus is involved in the exhibition of depression symptoms in adult rats, which could lead to the presumption this structure might also be responsible for such symptoms in the human amygdala (Figure 2) (Amaral & Adolphs, 2016).
Depression has also been linked to amygdala volume. In a meta-analysis of thirteen MRI studies done by Hamilton and colleagues (2009), between the years 1985 and 2008, it was found that patients with major depression tend to have a decrease in amygdala volume, and it was also observed that those depressed patients who took antidepressant drugs had amygdala sizes comparable to never-depressed individuals. This finding can be explained due to the fact that depression is a neurodegenerative condition which affects nervous tissue in all the brain, while antidepressant medication is neurogenerative and neuroprotective, hence the similar amygdalar volume size between those patients who take antidepressant medication and healthy ones.
Recent neuroimaging studies have found that neurological processes within the amygdala can be manipulated to decrease depressive symptoms. This research is essential, as the prevalence of drug ineffectiveness for major depressive disorder is high. In a double-blind, placebo-controlled, randomized clinical trial performed by Young and colleagues (2017), thirty-six right-handed adults of both sexes, between the ages of 18 and 55 years, diagnosed with depression and unmedicated, were randomly chosen to undergo two real-time functional magnetic resonance imaging neurofeedback (rtfMRI-nf) procedures, of either the left amygdala or the left horizontal segment of the intraparietal sulcus (a region not implicated in the regulation of emotions – the control group). In this kind of neurofeedback intervention, subjects were placed inside an MRI machine, and were shown an image of a thermometer presenting a value that would change in accordance their engagement in autobiographical recalling, hence controlling their emotions and enhancing the performance of their amygdalae in this manner. It was found that the mean scores of the amygdala rtfMRI-nf group on different depression inventories and scales (Beck Depression Inventory-II, Snaith-Hamilton Pleasure Scale, Montgomery-Åsberg Depression Rating Scale, Hamilton Depression Rating Scale, and the Autobiographical Memory Test) were significantly lower (p<0.05) with subsequent study visits (visit 1: baseline; visit 2: first rtfMRI-nf; visit 3: second rtfMRI-nf; visit 4: follow-up), in comparison to scores attained in the control group. Similarly, there was an evident decrement in the response to negative stimuli (which is usually exaggerated in depressed individuals), as well as an improved reaction to positive stimuli, and there was amelioration in the recall of emotionally-positive autobiographical memories, which is often defective in the depressed individual.
In light of the aforementioned research evidence that sets the amygdala as a brain structure of paramount importance in fear and anxiety regulation, emotional autobiographical recall, and cognitive processing, it is important that clinicians detect signs and symptoms that could suggest a deficit in its performance early in consultation, to then be able to indicate appropriate diagnostic and therapeutic techniques, such as rtfMRI-nf and antidepressant medication. As with current research on every cerebral structure and neurological process, studies on the amygdala still have much to unveil. For one thing, neuronal interconnections between the amygdala and other encephalic structures, like the occipital and frontal lobes, the hippocampus, and the thalamus, have not yet been entirely elucidated, to the point there is still discord on how to properly delimit different nuclei within the amygdala. Then, notwithstanding major progress in psychoactive drug development, antidepressant and anxiolytic drug specificity continues to be rudimentary, as adverse reactions are significant up to the present time, causing patient withdrawal from treatment schemes. Finally, there ought to be a greater governmental effort to implement better screening programs for depression and anxiety, especially for children and adolescents, and it would be of major social benefit to have widespread access to brain MRI scans, as many cerebral abnormalities (including amygdala deficiencies in volume, structure and blood perfusion) will not be detected during clinical evaluation until in advanced stages, where treatment may need to be more complex and expensive.
References
Amaral, D.G & Adolphs, R. (2016). Living without an amygdala (1st edition). New York, NY: The Guildford Press.
Comer, R.J. (2015). Abnormal Psychology (9th edition). New York, NY: Worth Publishers.
Forster, G.L., Novick, A.M., Scholl, J.L. & Watt, M.J. (2012). The Role of the Amygdala in Anxiety Disorders. The Amygdala – A Discrete Multitasking Manager. doi: 10.5772/50323
Hamilton, P., Siemer, M. & Gotlib, I.H. (2008). Amygdala volume in Major Depressive Disorder: A meta-analysis of magnetic resonance imaging studies. Molecular Psychiatry. 13(11), 993–1000. doi:10.1038/mp.2008.57.
Young, K.D., Siegle, G.J., Zotev, V., Phillips, R., Misaki, M., Yuan, H., Drevets, W.C., Bodurka, J. (2017). American Journal of Psychiatry. 174(8), 748-755. doi: 10.1176/appi.ajp.2017.16060637.