Gout = inflammatory response to excess amounts of uric acid (UA) in the body resulting in acute attacks of arthritis.
UA = byproduct of purine metabolism, normally excreted by kidneys
- At low levels, UA = important antioxidant
- At higher levels, UA = pro-oxidant, pro-inflammatory
If hyperuricemia continues, chronic illness will develop that is characterized by the presence of inflammatory nodules in the joint and subcutaneous tissue, severe pain, limited movement, and grotesque deformity.
Clinical manifestations
- hyperuricemia
- recurrent attacks of acute gout limited to one joint
- monosodium urate (MSU) crystals form tophi in and around the joints
- renal disease
- formation of MSU renal stones
Three clinical stages
- asymptomatic hyperuricemia – may go unnoticed, may persist throughout life if disease does not progress
- acute gouty arthritis – acute attack of pain, heat, swelling, and erythema localized to one joint
- tophaceous gout – progressive tophi deposition in cartilage, tendons, synovial membranes, and soft tissues

Figure 5. Tophaceous gout (Johns Hopkins Arthritis Center, 2019.)
Pathophysiology
Over time, elevated ↑UA → formation and deposition of monosodium urate (MSU) crystals
- In and around joints
- In subQ tissues
- In kidneys
MSU crystal deposition causes
- Cytokine-mediated inflammatory response characterized by
- Release of TNF-α
- Release of chemokines and interleukins
- Initiation of complement system
- Triggers activation of macrophages and neutrophils
- Release of cellular contents exacerbates inflammation
 Figure 6. Gout pathology (Journal of Advanced Research, 2017).
Figure 6. Gout pathology (Journal of Advanced Research, 2017).
- Release of cellular contents exacerbates inflammation

Long-term accumulation of MSU crystals results in
- Gouty arthritis – ranges from acute attacks of monoarticular arthritis to chronic arthritis characterized by permanent joint damage
- Tophi – small, white, nodular crystal deposits in subcutaneous tissues
- Renal calculi
- Acute nephropathy resulting from crystal deposition in renal tubules
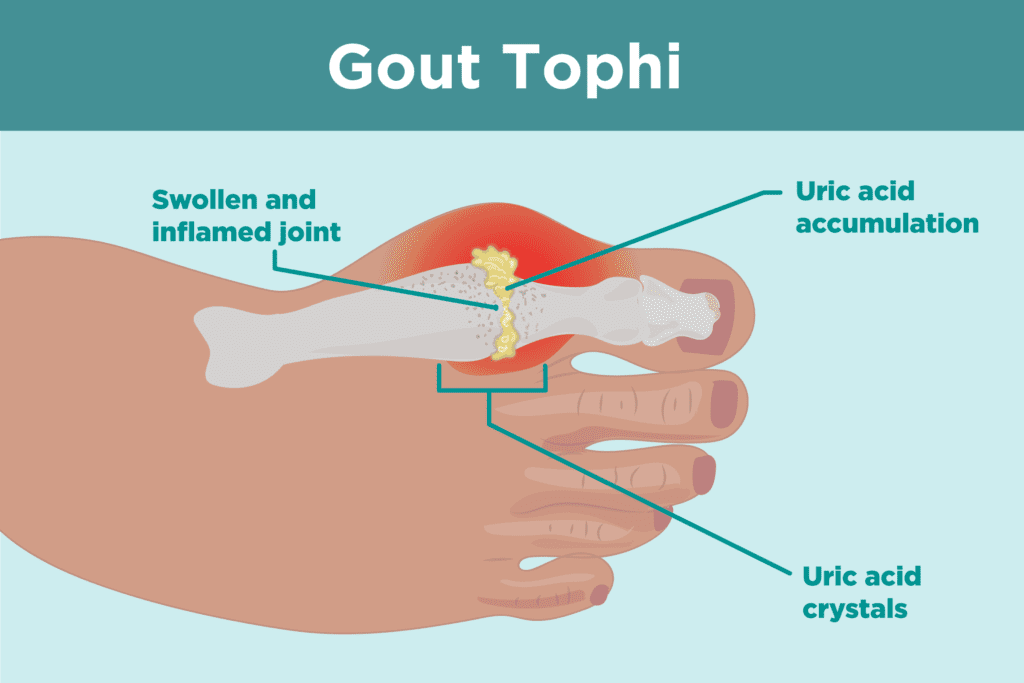
Figure 7. Gout Tophi (Barbara Brody, 2019).
CKD ⇔ gout
Primary gout – underexcretion or overproduction of ↑UA caused by an unknown metabolic defect
- Majority of individuals with gout have primary gout
Secondary gout – underexcretion or overproduction of ↑UA due to known etiology
- Accelerated rate of purine synthesis
- Accelerated rate of purine catabolism
- Genetic deficiency in HGPRT enzyme
- Lesch-Nyhan syndrome – X-linked genetic disorder, complete absence of HGPRT