https://www.youtube.com/watch?v=UXPXvSll3L4
Pathophysiology
The endometrium is the mucous membrane layer that lines the inside of a female’s uterus. This is the portion of the uterus that changes throughout the menstrual cycle, becoming thick and rich with blood vessels to prepare for pregnancy, then shedding if the woman does not become pregnant (Burney & Giudice, 2012).
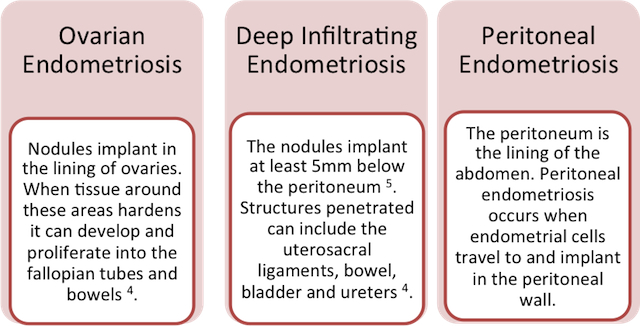
Endometriosis is defined as the presence of endometrial glands and stroma in ectopic locations, or locations other than the interior of the uterus. Primarily these locations are found to be the pelvic peritoneum, ovaries, and rectovaginal septum. Endometriosis is a chronic inflammatory, estrogen-dependent disease where ectopic implantations lead to an inflammatory reaction that may result in scar tissue (Burney & Giudice, 2012).
Bleeding during the menstrual cycle causes inflammation, which triggers cytokines, chemokines, growth factors, and protective factors to migrate to the area. The inflammation can lead to fibrosis, scarring, adhesions, and pain. Endometriosis is one of the leading causes of chronic pelvic pain and infertility in reproductive-age women, regardless of ethnicity or socioeconomic status (Bloski & Pierson, 2008).
Theories
There is no unifying theory regarding the origin of endometriosis. Rather, several theories have been proposed and researched:
- Sampson’s theory: endometrial cells reflux through the fallopian tubes into the abdominal cavity, leading to implantation onto the peritoneum. While widely accepted, this cannot be the sole cause of endometriosis because a majority of women experience some degree of retrograde menstruation, however few develop endometriosis (Mao & Anastasi, 2010).
- Celomic metaplasia: celomic cells, which differentiate from peritoneal cells, become endometrial cells that respond to triggers such as menses, toxins, or immune factors in a cyclic manner (Mao & Anastasi, 2010).
- Vascular and lymphatic spread: endometrial tissue infiltrates the local blood supply and lymphatic systems, and subsequently travels to distant sites in the body. This could explain how endometriotic implants migrate to locations such as lungs, bone, and skin. However, this theory does not account for gravity-dependent locations of implants, which constitute the majority of distant endometriotic implants (Bloski & Pierson, 2008).
- Altered immunosurveillance: endometriosis occurs either when the immune system is overwhelmed by menstrual back flow, or when a defective system allows the lesions to escape immunosurveillance, establish a blood supply, and continue to thrive.
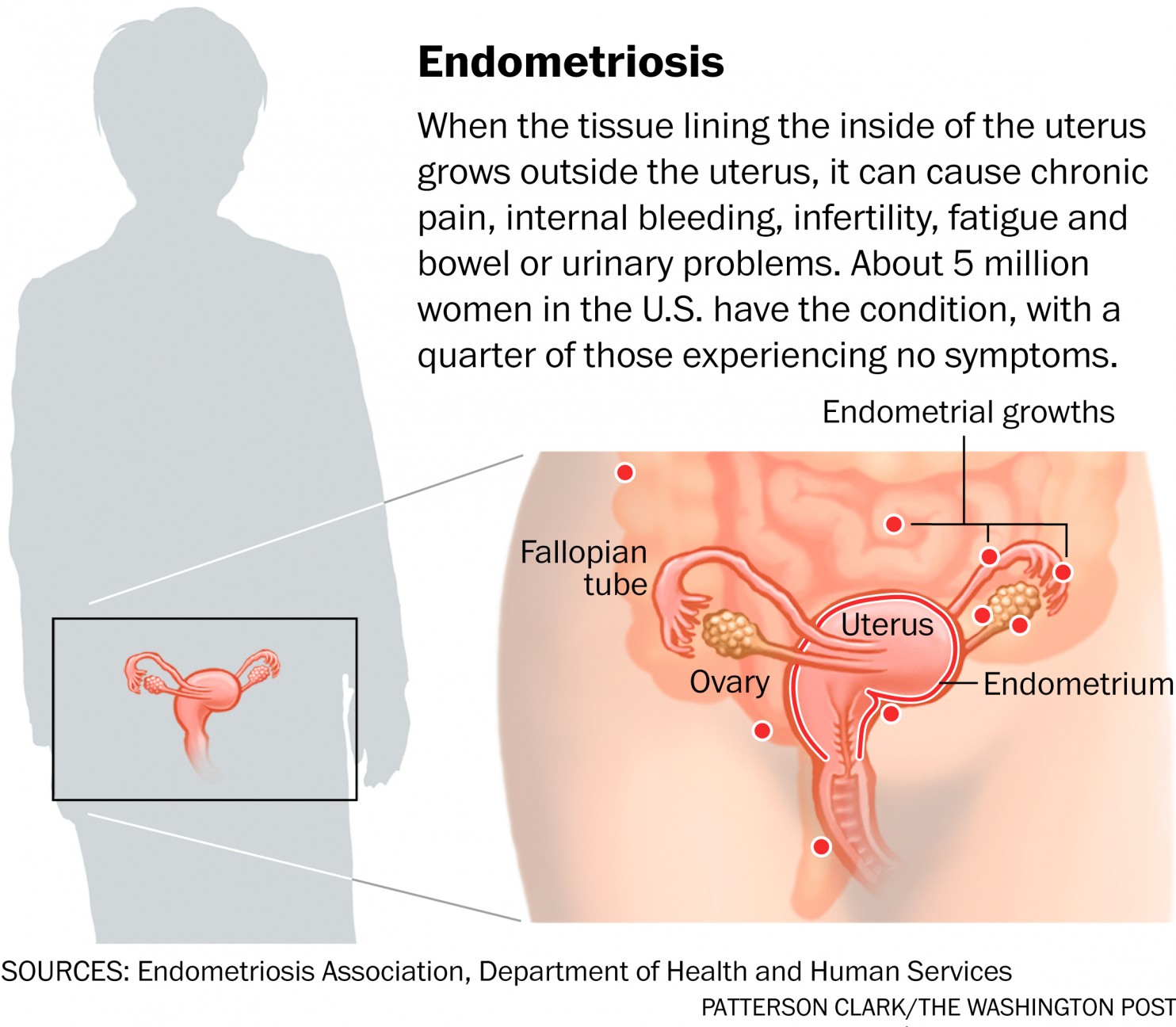
Photo from https://www.washingtonpost.com/national/health-science/for-women-with-endometriosis-answers-are-few/2015/05/04/c925edf2-c737-11e4-aa1a-86135599fb0f_story.html
Clinical Presentation
The clinical presentation of endometriosis varies greatly in severity, symptoms, and impact on the physical, social, and mental health of the woman. Determining diagnosis based soley on clinical presentation is challenging due to the wide range of symptoms, which can often overlap with several other gynecologic and nongynecologic conditions, including chronic pelvic inflammatory disease and irritable bowel disease (Mao & Anastasi, 2010).
Typical presentation includes:
- Chronic pelvic pain (> 6 months, most common sx)
- Tends to increase in severity premenstrually then subside with menses cessation (Mao & Anastasi, 2010)
- Dysmenhorrhea
- Dyspareunia
- Lower back pain
- Dyschezia
- Dysuria
- Infertility
A note on pelvic pain:
Interestingly, the objective signs and subjective symptoms associated with pelvic pain do not always correlate. Patients presenting with minimal disease may have debilitating pain, whereas other clients with severe stage III–IV disease are asymptomatic (Hsu et al., 2010).
I’m medical student