(VoiceThread should be 1-2 minutes long and describe the normal physiology as well as the pathophysiology of the chosen diagnosis.
(NOTE: The example provided below does NOT include normal physiology and would not be scored a 100%)
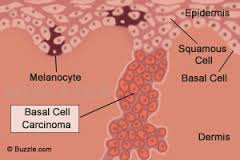
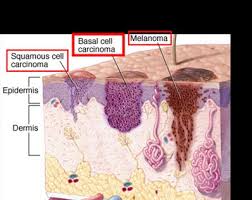
Basal cell carcinoma (BCC), the most common type of skin cancer, arises from undifferentiated basal keratinocytes of the epidermis, hair follicles, and eccrine sweat ducts (McCance & Huether, 2014). Histologically, the cells are basophilic with large nuclei. The incidence of BCC cases is increasing, probably because of changes of leisure activities and migration to regions with higher solar radiation. BCCs rarely metastasize (< 0.1%), and mortality rates are low; however, some tumors grow aggressively and may cause extensive tissue damage (e.g. destruction of nose, ear, eyelid) if they go untreated (Berking, Hauschild, Kolbl, Mast & Gutzmer, 2014). Because basal cell carcinoma requires surrounding stroma for support during growth, it does not metastasize via blood or lymphatics. Ultraviolet (UV) radiation exposure is by far the primary cause of BCC, but this skin cancer is also associated with certain physical characteristics such as fair complexion, red or blond hair or light eye color, exposure to arsenic, coal tar derivatives, irradiation, and the autosomal dominant nevoid basal cell carcinoma syndrome (McCance & Huether, 2014 ). Mutations in the TP53 tumor-suppressor gene as a result of UV radiation exposure or other carcinogenic factors lead to a deficit in keratinocyte repair function and apoptosis resistance of DNA-damaged cells. Other mutations associated with BCC occur in the PTCH1 gene (tumor-suppressor activity) and changes in the Sonic Hedge-hog signaling pathway genes (responsible for protein coding essential for cell growth and differentiation) (McCance & Huether, 2014; Berking et al, 2014).
BCC subtypes include superficial, nodular, and sclerosing/morpheaform (pigmented or nonpigmented). BCC lesions often appear first as a slightly elevated nodule, ivory in color with telangiectasis. Upward and lateral growth may occur and/or downward growth to the dermal-epidermal junction. Depressed centers and rolled borders are characteristic of BCCs and as lesions increase in size they will usually ulcerate, develop crusting and be firm to the touch.

http://www.basalcellcarcinoma.info/what-is-basal-cell-carcinoma