1.3: Use the best available information to develop patient care plans that reflect cost-effective utilization of diagnostic tools and therapeutic interventions appropriate for each unique patient and/or patient population and that are delivered in a compassionate, safe and error-limited environment.
Over the last few months, I had the opportunity to travel all across the country to interview for an orthopaedic surgery residency position. During one such interview, I remember sitting down with the program director and being asked to draw my favorite bone on the white board. I quickly drew my best representation of a femur, only for the PD to sarcastically comment about how that may be the most dysplastic femur he has ever seen. We then spent the next few minutes talking about what surgery I would do for each type of hip fracture that he drew. His last question to me was about how I would treat a sub-capital femoral fracture in a hospice patient. Confidently, I answered that I would do a hemi-arthroplasty given that it’s a faster operation with less morbidity, and in the past we used this implant in patients who were expected to live for less than a year. The PD paused and asked what else I could try. I responded maybe a short nail vs cannulated screws. He smirked and questioned if we really needed to operate on this patient. Would a surgery actually improve this patient’s quality of life? I vividly remember this encounter because it emphasized the importance of value based care. Weeks after this interview I continued to reflect back on my medical school experience to identify other lessons I learned about value based care and personalized medicine.
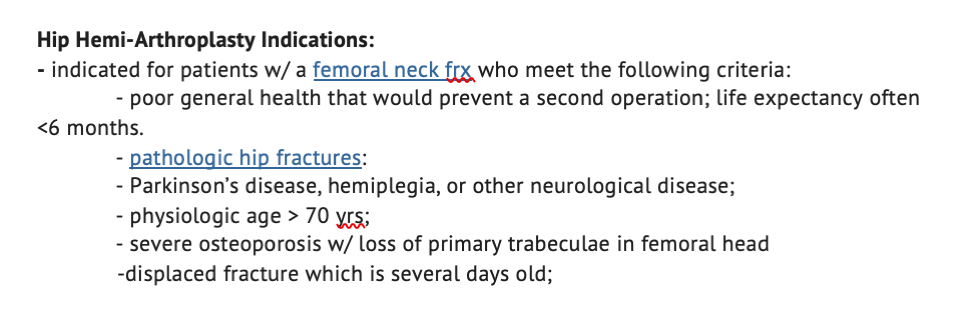 Artifact 1: Indications for a hip hemi-arthroplasty
Artifact 1: Indications for a hip hemi-arthroplasty
As a medical student during my pre-clinical years, I spent a majority of my time learning the various differentials for common complaints and almost memorizing diagnostic algorithms. When I saw a patient in LP, during an OSCE, or at the Columbus Free Clinic (CFC) I would refer back to my algorithms to ask almost a series of checklist like questions and order a pre-meditated battery of tests. One of my first reflective posts captured this attitude of viewing each encounter as a series of questions that had to be asked to do well (screenshot below).

Artifact 2: Part 1 portfolio post excerpt
This very algorithmic approach to medicine was called into question during one volunteer shift at the CFC. I had a routine patient coming in with Diabetes. During the visit I counseled the patient on the importance of eating well, exercising, checking sugar levels regularly, taking meds and consistently seeing us. I also ordered basic lab work (Chem to check for renal function, A1c, etc.), referral to ophthalmology for an eye exam, and did a diabetic foot exam. The staff physician after listening to my plan applauded my thoroughness but asked if I thought this was plausible for this patient. I was confused and didn’t understand what the physician was alluding to, and asked him for clarification. He explained that in this underserved population, the patients usually don’t have the resources to purchase a glucometer, medications and often don’t have a consistent method of transportation to attend all of these appointments. As a result, we must do as much as possible at today’s visit and provide the patient with all of the required education and medications. Experiences like this motivated my community health education (CHE) project at the CFC, which was a comprehensive longitudinal diabetes program. Each newly diagnosed diabetes patient received glucometers with strips, formal standardized education about the disease, dietician follow up at the CFC, access to CFC sponsored fresh produce, long term supply of medications and other services to help each patient. The artifact below is our group presenting this poster. From these experiences, I learned that each plan must be uniquely tailored to each patient and socioeconomic constraints of each patient must be taken into account to prevent the inefficient use of valuable health care resources.
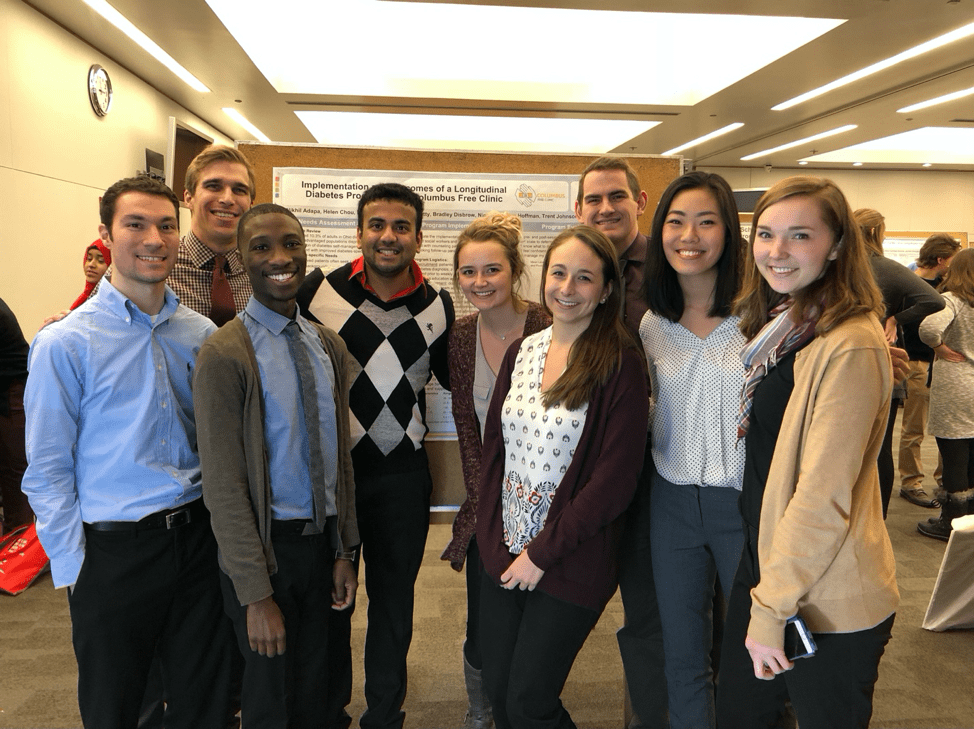
Artifact 3: CFC steering committee presenting CHE poster.
Overall, my experiences at the CFC and during my interviews this year have drastically reshaped my perspective on how medicine should be practiced. I am hoping to transition from the algorithmic style of medicine I was accustomed to early on in my career, to a more valued based individualized style. In my past few rotations, I have had extensive conversations about the appropriateness of antibiotics in chronic wounds, use of d-dimer in the ED, and whether an ammonia level is actually clinically warranted for a diagnosis of hepatic encephalopathy. These conversations have further shaped my practice. The final artifact below from recent evaluations showcase my newfound interest in value/evidence based care.
![]()
Artifact 4: Evaluation comments from last rotation
As a resident, I want to continue to develop these value based care principles. One of my goals for the future, is to consistently question why we are doing something for a patient and probe my attending surgeons for why we do things in a certain way. These conversations will better influence my future practice styles. After my interview day experience outlined previously, I hope to not use textbook indications for surgery to force surgery on my patients. Instead, I want to have an open conversation with my patients about their preferences and take into account their unique characteristics.